

Debunking Every Myth You Hear Against Universal Healthcare
Whether you are politically left or right, you should want Universal Healthcare as a human right—here are the receipts on why

On May 20, 1962, JFK delivered an impassioned speech at Madison Square Garden in favor of universal healthcare. Then, decades later in 2006 nearly 7 in 10 Americans believed the government should fund healthcare. And now, a new Gallop Poll reports that 62% of Americans believe in guaranteed universal healthcare. And despite this decades of support, not a single Presidential candidate this cycle had the courage to run on this wildly popular platform. Over the last week I’ve written in detail about America’s Violent Health System, and likewise, shared a deeply personal story about When Insurance Rejects Life Saving Care about our daughter Hannah Noor.
In response, I’ve received overwhelming empathy and compassion from conservatives and liberals alike, Republicans and Democrats, from those who self-identify as “Ultra MAGA” to those who label themselves as “Bernie Social Democrats.” Americans get it. Healthcare needs to be a human right.
Sadly, politicians, Republicans and too many Democrats alike, don’t get it. They worship at the altar of corporate donations. The health insurance industry annually spends a harrowing $700,000,000 on lobbying politicians to do their bidding. And that doesn’t even include what they spend on SuperPACs to block out candidates who dare run on a platform of guaranteed universal healthcare. Those same healthcare corporations then engage in a mass media blitz of misinformation and disinformation to convince people to vote against their own self-interests. In reality, guaranteed universal healthcare is a proven model adopted by every single developed nation on Earth (and many lower income developing nations). And while I do not have $700,000,000 to counter the lobbying propaganda health insurance corporations infuse into our politics, I do have access to the facts that health insurance corporations hope the American people don’t realize.
Below I address five of the main arguments against universal healthcare in the United States, debunk them with facts, and hope you feel compelled to share this far and wide with your networks. We can achieve healthcare as a human right in this country, but it requires us activating, organizing, and educating ourselves to successfully achieve that needed transformational change. Let’s Address This.

Myth 1: We Can’t Afford Universal Healthcare
Fact: The opposite is true. Dozens of studies prove that universal healthcare will save Americans billions of dollars annually. In fact, 22 studies reviewed all concluded that universal healthcare would save approximately $450 billion a year. And this is a universal conclusion. For example, “Even the Mercatus Center, a right-wing think tank, recently found about $2 trillion in net savings over 10 years from a single-payer Medicare for All system. Most importantly, everyone in America would have high-quality health care coverage.”
Moreover, we cannot forget that right now approximately 73 million Americans are on Medicaid, 68 million Americans are on Medicare, and 10 million Americans are on Tricare. That means that of our nation’s 335 million people, approximately 151 million are already on a universal (or near universal) healthcare model. And guess what? These programs each cost significantly less than the exploitative for-profit healthcare model. The overhead on these programs is 2-3%, while the overhead on for profit healthcare is 20%, plus a near unlimited mark up on prescription drugs. In this we have a side by side comparison of access to the exact same doctors and medications, except one has a nominal mark up and the other has a 10X markup. It doesn’t take an MBA in finance to understand that the same product or service without the massive markup is the smarter path to take. The only thing we cannot afford is for the current exploitative for profit model to continue.
Myth 2: If Costs Go Down, So Does Quality of Care
Fact: This is simply not true. It is important to understand why costs decrease, because contrary to the myth, every single one of the above studies found that quality of care would not decrease with universal healthcare. Costs under a universal healthcare model decrease instead because we stop wasteful spending. As consumer rights activist and scholar Diane Archer further explains in a point I reference above:
Medicare for All is far less costly than our current system largely because it reduces administrative costs. With one public plan negotiating rates with health care providers, billing becomes quite simple. We do away with three-quarters of the estimated $812 billion the U.S. now spends on health care administration. Administrative costs are so high because thousands of insurance companies individually negotiate benefit rules and rates with thousands of hospitals and doctors. On top of that, they rely on different billing procedures — and this puts a costly burden on providers.
Under a universal healthcare model the doctors that exist now would still exist. The medicine that exists now would still exist. The only thing that wouldn’t exist are the ridiculous and pointless administrative costs from for profit insurance corporations. Universal healthcare does not cut out healthcare itself, it cuts out the pointless middle man insurance corporation, and that is what save costs. In fact, speaking of high quality of care, a Yale study found that if we had universal healthcare during the pandemic, we would have saved more than 335,000 lives.
Myth 3: Universal Healthcare Puts Millions Out of Work
Fact: What would happen to the roughly 1.8 million Americans who work in medical billing? This is a great question and has a robust answer that I break down in three parts.
First, remember that about 40% of these jobs are already in the Medicaid and Medicare and Tricare industries—which is essentially universal healthcare for a portion of society. Therefore, we’re talk about roughly 1 million jobs, which admittedly is still a large number. What to do with those?
Well, hence the second point. Expanding Medicare to accommodate another 175 million people will necessarily require medical billing professionals and administrators to do those jobs. Therefore, the question is not about eliminating jobs, but about transitioning workers from the for profit exploitative system, to a non for profit system that prioritizes access to healthcare. Likewise, remember that ending the for profit system saves us at least $450 billion annually. These resources give us options. For example, these are excellent resources that could be spent on a lengthy 2-year salary severance to those in medical billing who do lose their jobs, plus adequate funding and training to allow them to become proficient in a new job. Indeed, at $70 billion annually, four-year-public college costs a fraction of what would be saved by shifting from an exploitative for profit model, to a universal healthcare model. We cannot afford not to make the shift.
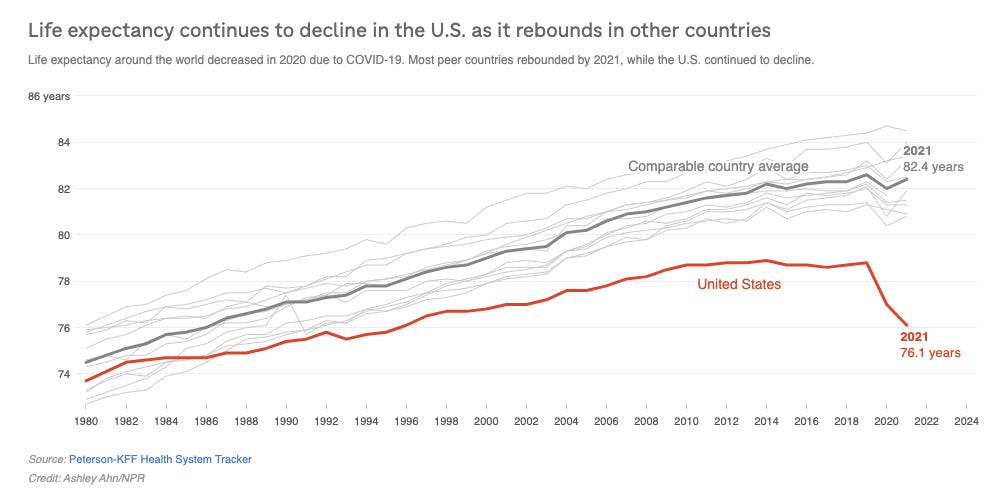
Finally, let us agree that maintaining an industry despite the harm an industry is causing is not a great argument. As The Lancet documents, the current for profit exploitative model enables 68,000 annual preventable deaths. The current for profit exploitative model results in the lowest life expectancy in the developed world, and declining, the highest infant mortality in the developed world, and increasing, and the highest maternal mortality in the developed world, and increasing. The current for profit exploitative model results in 500,000 medical bankruptcies every single year. Are 680,000 preventable deaths and 5 million medical bankruptcies over the past decade, and the daunting reality of another 680,000 preventable deaths and 500,000 medical bankruptcies over the next decade, really worth maintaining an industry that enables these atrocities—especially when better alternatives exist?
Myth 4: Universal Healthcare Means Tax Hikes
Fact: Universal healthcare means more money in your pocket. Insurance corporations want working people to pretend the exorbitant fees they charge for limited coverage does not come out of the same paycheck from which our taxes are withdrawn.
Studies show that Americans spend at least 18.7% of their income on healthcare costs. But even this is not a true picture because those who are lower income pay a disproportionately higher amount of their income to cover their healthcare costs. The Rand study on this subject reports:
Households in the bottom fifth of income groups pay an average of 33.9% of their income toward health care, while families in the highest-income group pay 16% of their income toward health care. The analysis finds that households in the middle three income tiers pay between 19.8% and 23.2% of their income toward health care.
Here’s why these numbers matter. There does not exist a universal healthcare model that increases taxes by 33.9%, or 23.2%, or even 18.7%. It simply does not exist. Even if income taxes dramatically increase from 24% to 34%, that is still a net savings of 8.7%-23.9% on overall take home pay. University of California, Berkeley professors of economics Emmanuel Saez and Gabriel Zucman illustrate this well:
Take the case of a secretary earning $50,000 in wage and currently contributing $15,000 through her employer to an insurance company. With universal health insurance, her wage would rise to $65,000 – her full labor compensation. With an income tax of 6% – which, if applied to a base large enough, would be enough to fund universal health insurance – she would have to pay about $4,000 more in tax. But the net gain would be enormous: $11,000. Instead of taking home $50,000, the secretary would take home $61,000.
And moreover, this new model would ensure she pays no more deductibles, co-pays, or additional out of pocket costs. Why? Because the universal healthcare model is designed to maximize access to healthcare, not maximize profits for billion dollar corporations.
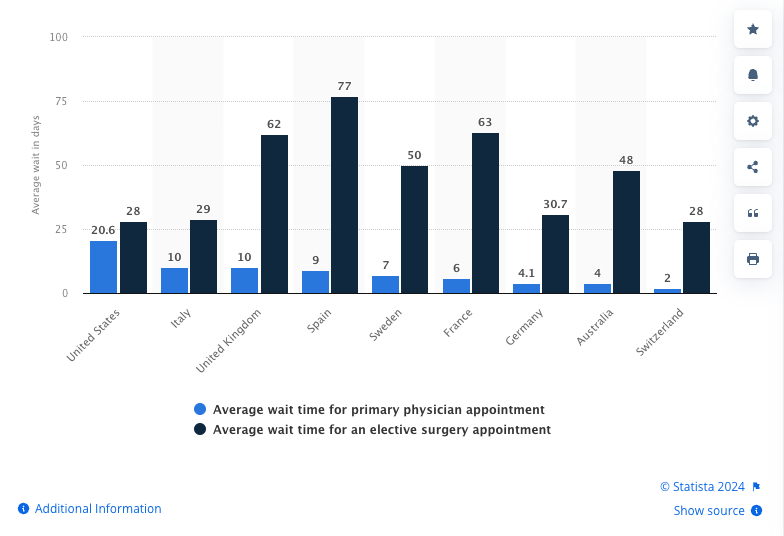
Myth 5: Universal Healthcare Causes Long Wait Lines
Fact: For primary physician appointments, Americans already wait longer under our exploitative for profit model than do people in nations with universal healthcare. Frankly, I marvel at this allegation as I reflect over the fact that it took us more than two years to get our daughter the critical life saving medication she needed, only because our exploitative for profit health insurance company refused to accept our doctor’s medical instruction. In reality, wait times in the United States are shorter only for elective surgery, but for primary care or for critical care, the United States is the worst out of any nation with universal healthcare.
Moreover, think about how illogical the claim is that universal healthcare results in wait times that hurt our health. If that were true, why does every developed nation have a higher life expectancy than does the United States? Why do each of them have lower maternal mortality than does the United States? Why do each of them have lower infant mortality than does the United States? Why why do none of them have medical bankruptcy, while we have 500,000 annually? None of this is by accident. It is due to the obvious fact that when healthcare access is dependent on ensuring people are healthy, rather than on seeing people as piggy banks, healthcare is administered faster.

And for those who claim that universal healthcare is economically unsustainable, and point to the struggles of the British National Health System (NHS), I remind them that any system that is not properly funded will collapse. A recent detailed analysis by the New England Journal of Medicine reports that the main reason why the NHS is struggling has nothing to do with access or quality of care, but instead that, “The primary contributor is long-term underinvestment in health services.” Again, this is not accident, but a choice by right wing politicians.
Right wing politicians in the UK are working hard to convince the British public that America’s for profit model is the promised land in healthcare access. Our neighbors across the pond should know they’re being sold rubbish (as I’m told they say over yonder) and not to believe a word of such corporate funded propaganda.
Bonus Myth: Why Should I Pay For Other People’s Healthcare?
Fact: How do you think health insurance works? Once you figure that out, you’ll realize that you’re already paying for other people’s healthcare, as they are paying for yours. You’ll also realize that having a larger pool of money from which to cover costs for everyone actually saves you money. And finally, you’ll realize that because more than 75 million Americans are uninsured or underinsured, every time they can’t pay a bill, for profit insurance companies raise your rates to make up the difference. So when people don’t have healthcare, it costs you. Therefore, even if all you care about is yourself, you should want everyone to have healthcare because it will lower your costs as well.
Conclusion
As I posted on BlueSky, “If the killing of the UnitedHealth CEO has taught us one thing, its that we're maybe not as divided as we think. When 90% of people empathize with the people the CEO exploited more than with the CEO, it should tell our politicians something. Stop bowing to billionaires & actually work for the people.”
The facts are clear. Universal healthcare costs less, renders the same high quality care, will save at least 68,000 lives annually, prevents 500,000 medical bankruptcies, ignites job creation, increases life expectancy, decreases infant and maternal mortality, and eliminates for profit health insurance lobbying, which is a major source of exploitative lobbying to America’s politicians. Literally the only people who believe we need to spend hundreds of billions on administrative costs are insurance executives who need that money for their precious private jets and yachts. I think I can speak for at least 99% Americans when I say, America will be better off with more healthcare access and few private jets for billionaires.
Despite how divided we seem as a nation, Republicans and Democrats alike are united in the need for healthcare as a human right, and we should remember that next time wealthy elites try to position us against one another.
P.S. If I missed a myth, share it in the comments and I’ll consider a future part two piece diving into those.
I'm a Canadian RN who worked for 20 years in a US Level I Trauma, County ER. County hospitals are America's socialized medicine in that they will see a patient and provide all the care that is needed, even as much as organ transplant, regardless of the patient's ability to pay. All i knew was care that was never restricted or profit focused. Then I made the unfortunate leap to the world of for profit, cooperate health care.
For profit health care is nothing short of evil. It is the reason that for the 5th year in a row US healthcare has ranked last amongst all developed nations in access, equity and outcomes. In our system you are more likely to die from a preventable medical error than from your admission diagnosis when admitted to a hospital. Nurses and Physcians are made to focus on cost saving metrics. The most harmful to patients metric that Provider's are forced to meet is "decrease length of stay." In the ER this metric is represented by a 90 minute time goal from door to disposition. Patients are rushed through emergency rooms so the that the next patient can be seen decreasing patients leaving without being seen. Every patient who grows tired of waiting and leaves an ER before being seen is lost revenue to the hospital. Emergency rooms have invented work arounds to capture this revenue. They will do such things as have a PA see the patient at triage and order labs or maybe even a CT while the patient is sent back to the waiting room. Since the patient was seen briefly by a mid level provider the hospital can bill the patient's insurance. The patient however, languishs in the waiting room awaiting an available bed in the back.
Once in the back the 90 minute clock starts ticking. Provider's are forced to consider the most likely diagnosis instead of the usual standard of care for the ER, and to utilize a high index of suspicion, ruling out threats to life. Thorough workups once standard to emergency rooms are no longer the standard because of the pressure to hurry patients through the ER to either an inpatient bed or to be discharged. I saw this result in many what the trade calls "bounce backs". Patients who would be discharged and return in extremis because all along they had a life threat.
Needless to say I did not do well as an ER nurse in the for profit setting. I could not bring myself to send people out the door that I knew needed further workup. I was counseled for exceeding my 90 minutes because I refused to put an elderly, confused man with a hip fracture in a wheelchair and sit him in the waiting room to await family that was two hours away. There was no doubt in my mind if I had put this older gentleman in the waiting room, alone that he would fall. And this time likely sustain a head injury and, possible brain bleed being that he was on anticoagulants. That was cooperate emergency room care.
A fairly good article, but let's go deeper.
I have proof that my Principal Care Physician makes medical decisions partly based on what my insurance company will cover. She has prescribed a diabetes system (strips, gauge, etc) from a particular company because my insurance company gives a co-pay of "only" 30 dollars for a month worth of strips. However an equally effective generic brand only costs 20 dollars a month retail, with no insurance coverage. When asked why she prescribed the more expensive system, it was because "your insurance covered it".
I needed a CPAP machine. She prescribed a model and outlet for the machine that was "covered" by my insurance because I had reached my deductible cap in a year. On January 1st, when the deductible was reset I found out that I was RENTING the machine for 200 dollars a MONTH. Online the machine cost 1000 dollars to buy. I returned the rental and bought the 1000 dollars machine (since reduced to 700 dollars to purchase) and have been using it for five years.
I do not believe my doctor is doing this out of corruption issues, but the insurance influence has to GO.
Another issue about our healthcare system is that companies use group health plans to capture and keep employees as benefits. If single-payer was to happen, companies would have to find some other way to find and keep employees.
Finally your article did not mention the gain in the economy when we have a healthier (and happier) workforce.